Total hip replacement surgery THR
In this article Dr. Pili explains total hip replacement surgery, addressing common questions about the procedure and its outcomes.
If your orthopaedic surgeon has recommended a total hip replacement (THR), don’t worry; despite how daunting it may seem, you are one of over 70,000 patients undergoing this treatment each year in Italy.
This procedure will improve your quality of life and has a success rate higher than most surgical interventions performed today.
Only coronary bypass surgeries have a higher outcome regarding the increase in quality of life.
Despite its success, total hip replacement surgery is a serious surgical procedure and should be regarded as such, as it presents both benefits and risks.
In this article, we hope to address most of the questions you may have regarding this operation and its effectiveness in treating hip osteoarthritis (coxarthrosis).


When do I need a THR?
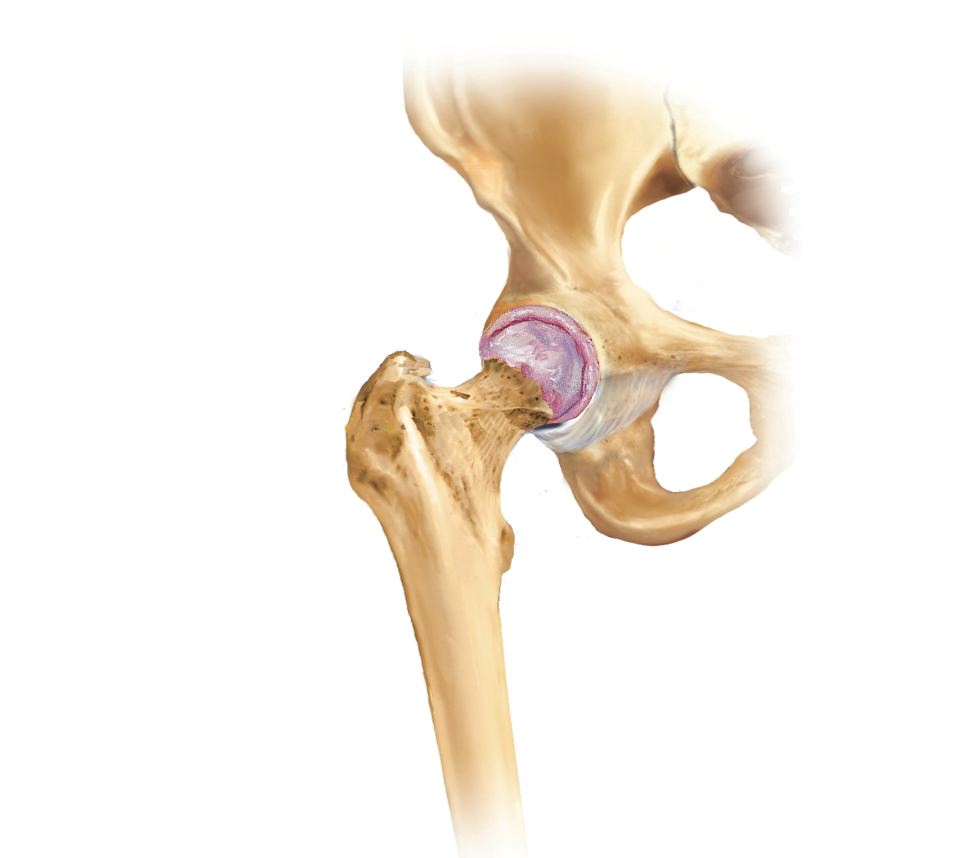
You may need a total hip replacement because the joint is damaged due to a condition. The hip joint is formed by a ball, the femoral head, that rotates within a socket called the acetabulum. During this procedure, both of these components are replaced. The total hip replacement surgery has a very high success rate. In fact, about 95% of patients who undergo this procedure (19 out of 20 surgeries) report significant improvement and are happy to have had the operation. This makes it one of the most successful surgeries.
What can I expect from a THR?
The greatest benefits of total hip replacement surgery include a drastic and almost immediate reduction in pain. Additionally, the mobility of the joint may increase, along with the ability to carry out daily activities with greater comfort. However, it is important to keep in mind that the new joint will never be as good as that of a healthy person and will have certain limitations.
What happens during total hip replacement surgery?
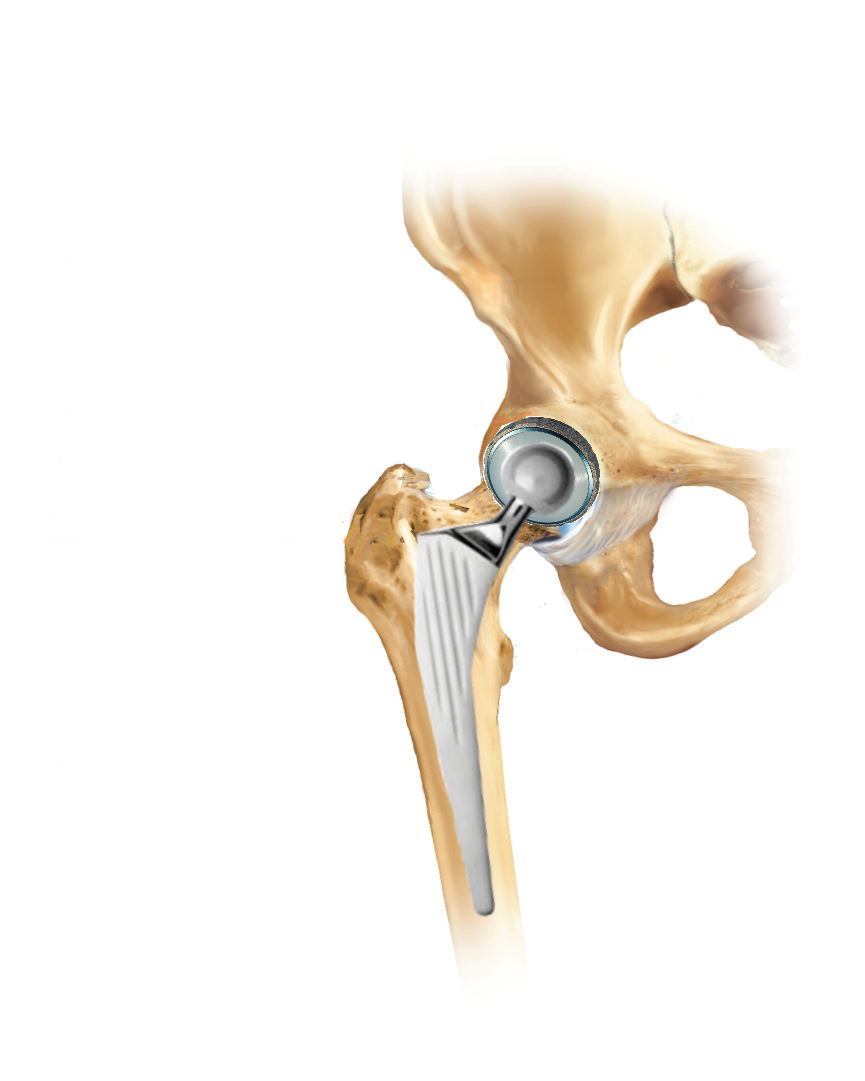
During the THR procedure, an incision is made along the lateral part of the thigh and buttock. The damaged joint is removed and replaced with an artificial prosthesis. Typically, the prosthesis consists of a metallic component for the femur and a polymethyl methacrylate (plastic-like) component for the socket. However, the materials can vary and are selected from patient to patient, which may include metal, polymethyl methacrylate, and ceramic; discuss this with your surgeon.
Are there risks and complications?
As with all surgical operations, there are risks and potential complications and this includes having total hip replacement surgery, and your orthopaedic surgeon will recommend this procedure only if the benefits far outweigh the risks.
If the joint is severely damaged or you have other serious health conditions, the risks may increase.
You can discuss this with your surgeon.
Possible complications include:
– Respiratory tract infections and surgical site infections: To reduce the risk, antibiotics are administered just before the operation, and the procedure takes place in a sterile environment. If these complications arise, they will be promptly treated. If a wound infection occurs, antibiotics or additional surgeries may be necessary, depending on the case.
– Deep vein thrombosis (blood clots in the venous system): Lower limb surgery can lead to deep vein thrombosis. To prevent this, an anticoagulant is administered for at least four weeks after the surgery to reduce the risk. Additionally, you will be taught exercises that also reduce the risk. Unfortunately, these measures do not completely eliminate the possibility of venous thrombosis or other types.
– Fractures: This complication is quite rare and is resolved in various ways depending on the circumstances.
– Prosthesis dislocation: This occurrence is relatively rare, and you will be instructed on how to avoid it. Occasionally, further surgeries may be needed to resolve the issue.
– Differences in limb length: Generally, this complication is resolved with an insole and is rarely noticeable or bothersome to the patient.
– Vascular or nerve damage: There is a slight risk of damage to nerves or blood vessels during the surgery. This complication is also rare and in most cases resolves spontaneously over time.
– Prosthesis mobilization: The prosthesis may become mobile and no longer remain fixed in its designated position, causing pain or may even dislocate. This usually occurs after several years and, in such cases, requires further surgery.
According to studies, prostheses that have not had complications are still well-fixed after 10-12 years in about 95% of cases and can last over 30 years.
Considering that they are mostly implanted at an older age, it is assumed that most prostheses will remain fixed for the duration of your life.
What can I do to reduce the risks of complications?
To reduce complications, it is essential to be in the best physical condition possible, thereby minimizing anesthetic and surgical risks. It is vital for anyone undergoing surgery to do their utmost to stay fit and to avoid risky behaviors. If you feel unwell or if your physical condition changes, you should inform your orthopaedic surgeon.
Can weight and diet influence the outcome?
If you are overweight, this condition will negatively affect the success of your surgery, so it is recommended that you lose weight before the operation. In fact, excess weight puts more strain on the prosthesis, reducing its lifespan. Excess weight also impacts anesthetic risk. If you are overweight, you should aim to reduce it prior to the surgery through diet and exercise.
Body Mass Index
The Body Mass Index (BMI) is calculated using your weight and height and helps determine whether you are overweight, of normal weight, or underweight. If your BMI is above 35, it means you are overweight, and in addition to needing to lose weight, you will require greater attention from the anesthetist. The same applies if your BMI is above 30 and you have other health conditions.
Smoking
We recommend quitting smoking or at least drastically reducing your smoking. Ideally, you should not smoke for at least a week prior to the surgery.
What is the preoperative visit?
Before the surgical procedure, you may be asked to have a preoperative visit to assess your health status and to undergo diagnostic tests.
What happens during the preoperative visit?
You may undergo an electrocardiogram and an X-ray of the affected hip and chest. Typically, your blood pressure, pulse, and body weight will be checked. Sometimes, blood tests may be required or existing tests may be reviewed. You will also be asked to undergo a urine test to diagnose possible urinary infections.
How long before the operation should I stop eating and drinking?
Before the surgical procedure, you will be asked to stop eating and drinking. This applies to the six hours prior to the operation. The reason for this is that consuming food or beverages can lead to regurgitation during the operation, causing severe anesthetic complications.
What happens on the day of admission?
On the day of admission, you will be invited to report to a designated area to complete various formalities. Please bring your medications and all relevant medical documentation, including X-rays.
What time will the surgery be?
The most appropriate time for your surgery will be determined by our medical team and will be confirmed the day before. This schedule is only indicative and may change on the day of the operation. In any case, you will be informed as soon as possible.
How will I prepare for the surgery?
You will be asked to remove your clothing, contact lenses, jewelry, watches, makeup, gel, fake nails, and nail polish. If rings cannot be removed, they will be covered with adhesive tape. Ideally, you should not bring any jewelry with you to the hospital. The area to be operated on may also be shaved.
If you have dentures, they will also need to be removed.
Can I take my medications before the surgery?
Yes, you should take your medications as usual. Some exceptions include medications like aspirin, clopidogrel, methotrexate, hormone replacement therapies, and oral anticoagulants (warfarin, acenocoumarol, etc.). Before stopping your therapy, consult your surgeon. If deemed necessary, the anesthetist may administer anti-anxiety medications shortly before the operation to help you relax.
Who will take me to the operating room?
A staff member will transport you to the operating theater on a stretcher or a wheelchair. You will be given appropriate clothing. At this point, some safety checks will be performed to ensure there are no errors before proceeding with the anesthesia.
What kind of anesthesia will I receive?
The type of anesthesia will be decided by the anesthetist in consultation with you, taking into account your specific needs. The main options will be general anesthesia or spinal anesthesia (epidural).
What happens at the end of the procedure?
After the operation, you will be kept in a safe area until the anesthetist is satisfied with your condition, at which point you will be returned to your room on the ward, where you will be monitored.
When will I recover from the anesthesia?
If you undergo general anesthesia, it is very likely that you will not remember much about what happens before you return to the ward. You will probably wake up with an oxygen mask, which will help you recover better from the anesthesia. You may also have an IV in your arm to keep you hydrated. You might have a pillow between your legs to prevent any movements that could jeopardize the prosthesis.
You will feel pain at the surgical site, but medications will be provided to reduce it. Ask the nursing staff for more pain relief if you believe it is necessary.
When can I drink or eat?
You should be able to eat or drink about an hour after the operation, provided you feel well and there are no specific instructions from your surgeon or anesthetist. After a few hours, you should be able to consume normal amounts of food, and you will need to make an effort to drink plenty of fluids to stay as hydrated as possible.
How can I go to the bathroom?
It is important that you go to the bathroom when you feel the need and allow the nursing staff to monitor you. If you are unable to urinate within 6-12 hours after the operation, you should inform the nursing staff, and they, along with the medical team, will decide what to do. If necessary, a urinary catheter will be placed. It is quite normal to experience constipation after the surgery. If this persists for more than two days and is causing you issues, a laxative may be administered.
What if I have trouble sleeping?
You will be offered and given pain relief medications. However, if this is not sufficient, do not hesitate to inform our nursing staff, who may administer additional medications if indicated.
What rehabilitation therapy will I undergo?
Rehabilitation therapy will begin immediately. You will be encouraged to perform exercises right away and to walk on the same day of the operation or the day after. Naturally, you will need to follow safety guidelines. The safety precautions you should observe include: do not flex the operated hip beyond ninety degrees, do not pick up objects from the floor without proper aids, do not cross your legs, and get out of bed with the operated leg first. Do not turn on yourself. You will be shown how to get in and out of bed, sit down, and get up from a chair and the bathroom to regain full independence as quickly as possible. You will be encouraged to walk with crutches on the same day of surgery or the next day, depending on your general condition. The mentioned safety precautions must be followed for three months after the operation. For this reason, you will need to make your home safe by obtaining devices such as seat risers and tools to help you manage your daily activities without risk.
What should I expect in the first six weeks?
Your hip prosthesis may dislocate, especially in the first six weeks, so you must adhere to all safety rules. In addition to those already mentioned, you should follow these additional precautions: sleep on your back, do not bend the hip beyond ninety degrees, and when in bed, sleep semi-reclined and never bend forward to touch your toes. Do not bend the operated leg to put on socks or shoes; always use the special aids. You should not sit on low seats that could cause your hip to flex beyond ninety degrees, but only on those with appropriate risers. The physical therapists will teach you how to perform common daily actions without risking complications, such as washing your feet and putting on socks and shoes.
What will happen to the surgical wound and the stitches?
The wound will be covered with a surgical dressing. It will be closed with stitches or staples. The stitches may need to be removed or may not, depending on the type used. If removal is necessary, it will be scheduled for 10 to 14 days after your surgery. The dressing must be kept dry until the wound is fully healed.
How long will I stay in the hospital?
Your average hospital stay will be 4-5 days. You will be able to go home when postoperative assessments have been completed and you are able to walk safely.
What clothes should I bring?
Bring comfortable and easy-to-wear clothing.
When can I go home after the surgery?
Your discharge will be decided by the medical staff.
If I need certifications?
Any necessary certifications will be provided at the time of discharge.
When can I drive?
You should not drive for at least six weeks after discharge, and even after this period, if you are not confident in your ability to perform the necessary maneuvers in an emergency. Check with your insurance to ensure you are covered.
When can I return to work?
This depends on your job. If your work does not require particularly strenuous tasks, you may be able to return around eight weeks. On average, most people return to work around twelve weeks.
How can I stay fit before the surgery to achieve the best possible outcome?
Staying fit before the surgery is very important. This will optimize the results of the procedure, recovery from anesthesia, and postoperative physical recovery. Engaging in physical exercise will help significantly, and upon request, exercises that can be done while watching television will be provided. Losing weight if you are overweight is equally important.
For further information, feel free to contact us using the form below.


